Dear All (prepare for something that is delightfully different and marvelously wonkish AND with thanks to Lance Price for co-authoring this newsletter),
Continuing with the theme in the 15 Aug 2025 newsletter (“Global livestock resistome: Antibiotic resistance is widespread!”) of ways to use sequencing of samples from the environment, we have today an amazing paper in Nature which shows that infections have been plaguing mankind for a long, long time:
Sikora, M., Canteri, E., Fernandez-Guerra, A. et al. The spatiotemporal distribution of human pathogens in ancient Eurasia. Nature 643, 1011–1019 (2025). https://doi.org/10.1038/s41586-025-09192-8.
In brief, the authors analyzed ancient human DNA for evidence of infectious diseases, creating a global infection map spanning spanning 37,000 years. At a more technical level, the process is well summarized by the opening lines of the abstract (line breaks added):
- “To create an archaeogenetic-based spatiotemporal map of human pathogens,
- we screened shotgun-sequencing data from 1,313 ancient humans
- covering 37,000 years of Eurasian history.
- “We demonstrate the widespread presence of ancient bacterial, viral and parasite DNA, identifying 5,486 individual hits against 492 species from 136 genera.”
You’ll want to spend some time with paper yourself, but let us intrigue you with the data on Yersinia pestis (aka, “the plague”) and Borrelia recurrentis (louse-borne relapsing fever). First up, these figures on Y. pestis:
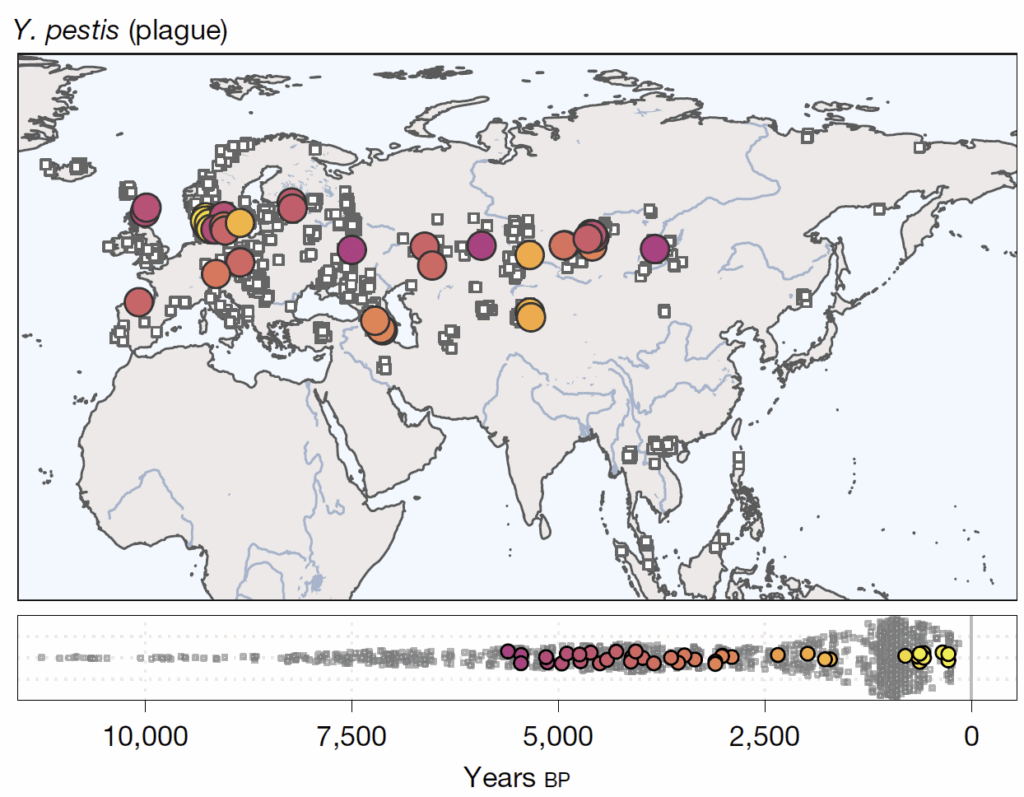
Look closely … there are 5 boxed figures and some x-axes stacked up here! They require careful study!
- The upper pair of figures (the map and the boxed figure below it) with the timeline x-axis running from 10,000 BP to 0 BP show the distribution across Eurasia of samples showing DNA for the plague.
- The authors do have data going back to 37,000 BP, but this analysis focuses on the most recent 10,000 years.
- Background BP = Before Present based on radiocarbon dating.
- By definition, 0 BP = 1950 AD.
- To convert to BC/AD (or BCE/CE), it helps to round a bit by envisioning the scale as running from -10,000 to 0 and then adding 2,000 … 10,000 to 0 BP is thus ~8000 BC/BCE to ~2,000 AD/CE.
- The light grey dots are the estimated date of the samples from the entire dataset of 1,313 individuals. The colored dots correspond to the dates of the plague-positive DNA samples.
- The authors do have data going back to 37,000 BP, but this analysis focuses on the most recent 10,000 years.
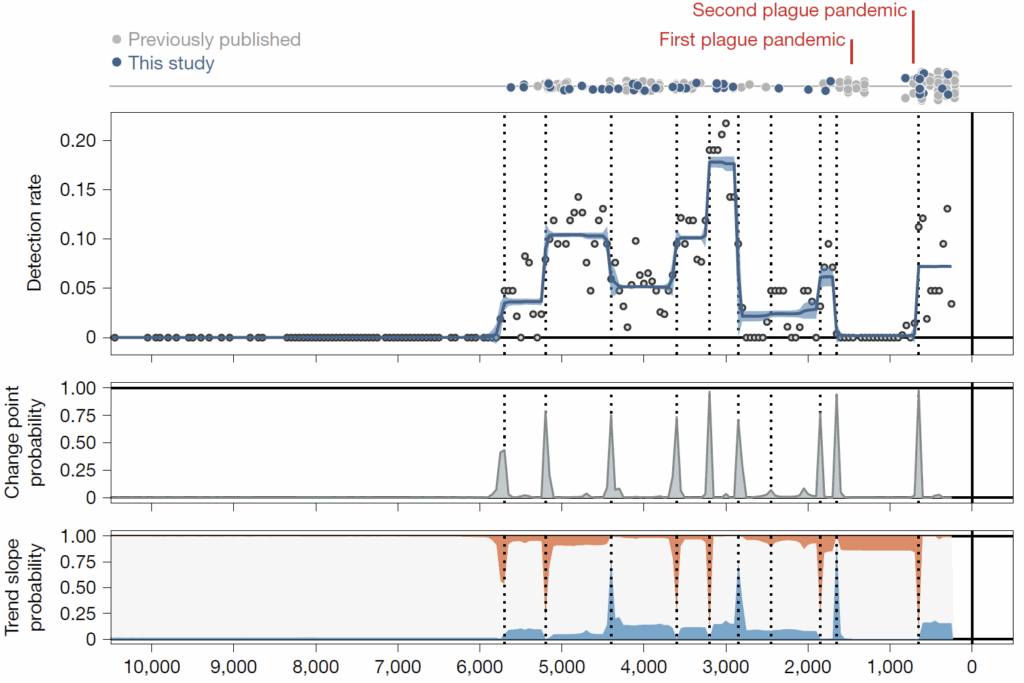
- Moving down, we have a trio of boxed figures that, importantly, share the same 10,000 BP to present (~8,000 BC to ~2,000 AD) timeline.
- Just above the first boxed figure of this trio, note the thin grey line with grey and blue dots. The authors are here combining their cases of plague (blue dots) with other published cases (grey dots).
- Then, the first boxed figure of the trio gives a grand roll up (blue line with y-axis labeled Detection Rate) of their best estimate of the timing of cases and hence timing of waves of cases.
- The two final boxed figures are the statistical analyses that underpin the Detection Rate estimate.
Impressive! The plague has come and gone over thousands of years! But interestingly, note that it didn’t become common until about 6,000 BP. And then please note the relatively low rates of plague in the periods 2,800-2,000 BP and then again 1,600-600 BP.
With those dates in mind, let’s now look at the same figures for louse-borne relapsing fever (LBRF). It may be less familiar than the plague, but it is also a deadly disease. Here we go:
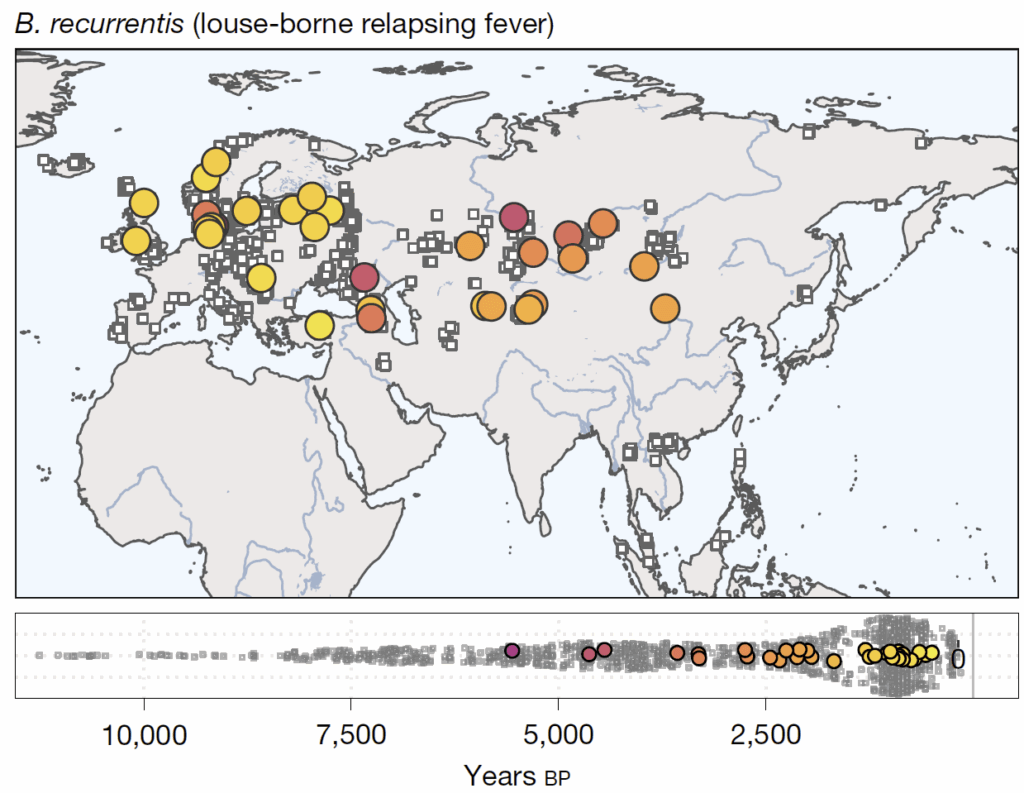
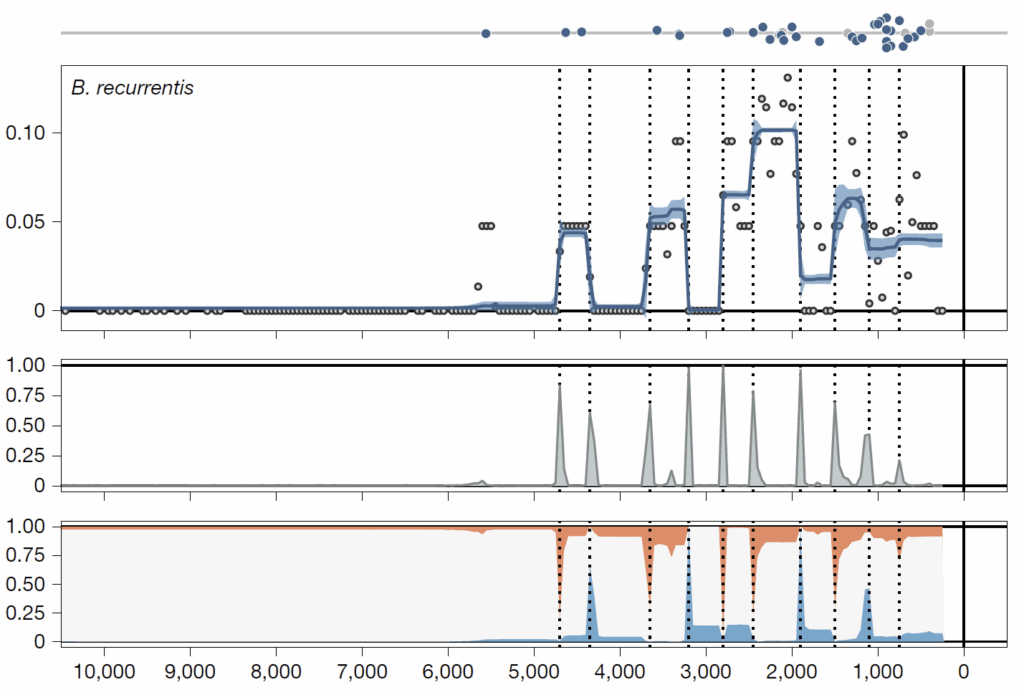
First, just absorb the general pattern for LBRF: As with the plague, there were no cases until ~6,000 to 5,000 BP then waves of cases thereafter. This timing is instructive … as the paper states, “A striking feature shared in the temporal dynamics of plague and LBRF was the absence of detectable cases before roughly 6,000 bp, coinciding with a transition of individuals in predominantly hunter-gatherer contexts to those in farming or pastoralist cultural contexts.”
Next, look at the two periods when plague was relatively quiescent (2,800-2,000, then 1,600-600 BP). Combined with evidence of steady rates of detection environmental pathogens (Fig. 5 in the ms if you want to follow along), this contrast of low rates of plague with the steady rates of LBRF cases is evidence that failure to observe cases of plague was not due to inadequate sampling but rather that the plague really did have have periods of relative quiescence.
—
Fascinating stuff, especially how closely the emergence of zoonotic diseases aligns with paleological estimates of livestock domestication. There’s more to explore in this paper (e.g., hints about leprosy, syphilis, and hepatitis B; cases of diphtheria from 11,000 BP; and more) and we’ll leave you to it. As you read, you might also enjoy the summary that includes some quotes from the authors in the 9 July 2025 New York Times.
And finally, this paper is evidence of the power of antibiotics and the many ways that their absence until about 80 years ago so often changed history. As the authors observe in their introduction:
- “Until around 1850, at least a quarter of all children died before the age of one, and around another quarter before turning 15.
- “Infectious diseases are estimated to have been responsible for more than half of these deaths.”
- Supporting citation: Volk and Atkinson, “Infant and child death in the human environment of evolutionary adaptation” Evolution and Human Behavior, 34:182-92, 2013, https://doi.org/10.1016/j.evolhumbehav.2012.11.007.
Please keep working on those new drugs! All best wishes, John & Lance
John H. Rex, MD | Chief Medical Officer, F2G Ltd. | Operating Partner, Advent Life Sciences. Follow me on Twitter: @JohnRex_NewAbx. See past newsletters and subscribe for the future: https://amr.solutions/blog/. All opinions are my own.
Lance B. Price, PhD | Co-director, Antibiotic Resistance Action Center | Professor, Milken Institute School of Public Health, George Washington University. E: lprice@gwu.edu; Twitter @battlesuperbugs. All opinions are my own.
John’s Top Recurring Meetings
Virtual meetings are easy to attend, but regular attendance at annual in-person events is the key to building your network and gaining deeper insight. My personal favorites for such in-person meetings are below. Of particular value for developers, the small meeting format of BEAM’s AMR Conference (March) and GAMRIC (September-October; formerly, the ESCMID-ASM conference series) creates excellent global networking. IDWeek (October) and ECCMID (April) are much larger meetings but also provide opportunities for networking with a substantial, focused audience via their Pipeline sessions. Hope to see you there!
- 1-3 Oct 2025 GAMRIC, the Global AMR Innovators Conference (London, UK). Formerly the ESCMID-ASM Joint Conference on Drug Development for AMR, this meeting series is now in its 10th year and is being continued under the joint sponsorship of CARB-X, ESCMID, BEAM Alliance, GARDP, LifeArc, Boston University, and AMR.Solutions. The ongoing series will continue the successful format of prior meetings with a single-track meeting and substantial networking time (go here to see details of the outstanding 2024 meeting).
- Registration is now open and the preliminary agenda can be found at that same link (https://www.gamric.org/). The meeting will be limited to approximately 300 attendees, so please be sure to register promptly to avoid disappointment!
- 19-22 Oct 2025 (Georgia, USA): IDWeek 2025, the annual meeting of the Infectious Diseases Society of America. Go here to register. For those who would like a substantial opportunity to present a product to a large audience (see also adjacent note about ESCMID), note the call for applications to present at an IDWeek Pipeline Session; go here to submit an application for your compound or diagnostic.
- 3-4 Mar 2026 (Basel, Switzerland): The 10th AMR Conference. Sponsored by the BEAM Alliance, the 9th AMR Conference has just concluded and it’s again been an excellent meeting! Please mark your calendar for next year. You can’t register yet, but details will appear here!
- 17-21 April 2026 (Munich, Germany): ESCMID Global 2026, the annual meeting of the European Society for Clinical Microbiology and Infectious Diseases. You can’t register yet, but you can go here for details on the outstanding 2025 meeting. For those who would like a substantial opportunity to present a product to a large audience (see also adjacent note about IDWeek), I know that the meeting schedule will again include Pipeline Monday; go here to see details from 2025.
Upcoming meetings of interest to the AMR community:
- 15-19 Sep 2025 (virtual): US CDC-sponsored the 9th Annual Fungal Disease Awareness Week (FDAW). Daily themed events include “Think Fungus” on 15 Sep, “Fungi are everywhere” on 16 Sep, and “Fungal diseases and drug resistance (19 Sep). Signup for the Mycotic Diseases Branch newsletter to stay updated.
- 1-3 Oct 2025 GAMRIC, the Global AMR Innovators Conference (London, UK; formerly the ESCMID-ASM Joint Conference on Drug Development for AMR). See list of Top Recurring meetings, above..
- 11-19 Oct 2025 (Annecy, France, residential in-person program): ICARe (Interdisciplinary Course on Antibiotics and Resistance) … and 2025 will be the 9th year for this program. Patrice Courvalin orchestrates content with the support of an all-star scientific committee and faculty. The resulting soup-to-nuts training covers all aspects of antimicrobials, is very intense, and routinely gets rave reviews! Seating is limited, so mark your calendars now if you are interested. Applications are being accepted from 20 Mar to 21 Jun 2025 — go here for more details.
- 17-20 Sep 2025 (Porto, PT): 14th International Meeting on Microbial Epidemiological Markers (IMMEM XIV). Go here for details.
- 9-13 Nov 2025 (Portland, OR, USA): ASM Conference on Biofilms. Go here for details and to register.
- 18-24 Nov 2025 (global, multiple locations): World Antibiotic Awareness Week (WAAW) is convened annually on 18-24 Nov by WHO with national events (e.g., CDC’s US Antibiotic Awareness Week (USAAW); ECDC’s 18 Nov European Antibiotic Awareness Day) occurring around the globe. Details will follow as events become visible.
- 19-22 Oct 2025 (Georgia, USA): IDWeek 2025. See list of Top Recurring meetings, above.
- 29-31 Oct 2025 (Bengalaru, India): ASM Global Research Symposium on the One Health Approach to Antimicrobial Resistance (AMR), hosted in partnership with the Centre for Infectious Disease Research (CIDR) at the Indian Institute of Science (IISc). Go here for details and to register.
- 28-30 Jan 2026 (Las Vegas, NV, USA): IDSA and ASM have announced a new US-based meeting series entitled IAMRI (Interdisciplinary Meeting on Antimicrobial Resistance and Innovation) and described as a “forum for collaboration and exploration around the latest advances in antimicrobial drug discovery and development.” You can’t register yet (the website says registration will open September 2025) but you go here for the program and to submit an abstract (deadline for abstracts is 1 Oct 2025).
- [NEW] 4-5 Feb 2026 (virtual, 8a-noon GMT on both days): Antimicrobial Chemotherapy Conference 2026, sponsored by BSAC and GARDP. Registration here: acc-conference.com. Abstracts are welcomed and can be submitted here; abstract deadline is Friday, 14 November 2025, 17:00 GMT.
- 3-4 Mar 2026 (Basel, Switzerland): The 10th AMR Conference sponsored by the BEAM Alliance. See list of Top Recurring meetings, above.
- 8-13 Mar 2026 (Renaissance Tuscany Il Ciocco, Italy): 2026 Gordon Research Conference (GRC) entitled “Antibacterials of Tomorrow to Combat the Global Threat of Antimicrobial Resistance.” A Gordon Research Seminar (GRS) will be held the weekend before (7-8 Mar) for young doctoral and post-doctoral researchers. Space for the GRS and the GRC is limited; for details and to apply, go here for the GRC and here for the GRS.
- 17-21 April 2026 (Munich, Germany): ESCMID Global 2026, the annual meeting of the European Society for Clinical Microbiology and Infectious Diseases. See Recurring Meetings list, above.
- 4-8 June 2026 (Washington, DC): ASM Microbe, the annual meeting of the American Society for Microbiology. The meeting format is evolving and next year will combine 3 meetings (ASM Health, ASM Applied and Environmental Microbiology, and ASM Mechanism Discovery) into one event. Go here for details.
Self-paced courses, online training materials, and other reference materials:
- OpenWHO: “Antimicrobial Resistance in the environment: key concepts and interventions.” Per the webpage for the course, it will teach you “…why addressing AMR in the environment is essential and gain insights into how action can be taken to prevent and control AMR in the environment at the national level.” This course builds on WHO’s 2024 Guidance on wastewater and solid waste management for manufacturing of antibiotics. For further reading, see also the 25 Sep 2023 newsletter entitled “Manufacturing underpins both access and stewardship: Cefiderocol as a case study” and the 28 Jan 2024 newsletter entitled “EMA Concept Paper: Guidance on manufacturing of phage products”.
- GARDP’s REVIVE website provides an encyclopedia covering a range of R&D terms, recordings of prior GARDP webinars, a variety of viewpoint articles, and more! Check it out!
- GARDP’s https://antibioticdb.com/ is an open-access database of antibacterial agents.
- The CARB-X website provides a range of recordings from its webinars, bootcamps, and more. A bit of browsing would be time well spent!
- British Society for Antimicrobial Chemotherapy offers an eLearning section: Education – The British Society for Antimicrobial Chemotherapy.
- NNF (Novo Nordisk Foundation) have announced their “Challenge Programme 2026 – Unravelling the Pathways of Human Invasive Fungal Diseases. The call seeks applications from EU-centered consortia (global partners are possible) for research in 4 areas: (i) fungal virulence factors, (ii) host-pathogen interactions, (iii) mechanisms of anti-fungal resistance, and (iv) fungal disease markers. Applications are due by 8 Oct 2025. Go here for details.
- ENABLE-2 has continuously open calls for both its Hit-to-Lead program as well as its Hit Identification/Validation incubator. Applicants must be academics and non-profits in Europe due to restrictions from the funders. Applications are evaluated in cycles … see the website for details on current timing for reviews.
- CARB-X will have two calls during 2025 that span two areas: (i) Small molecules for Gram-negatives (the focus is on Pseudomonas aeruginosa) and (ii) Diagnostics for typhoid (the focus is diagnosis of acute infections in 60 minutes or less). See this 26 Feb 2025 newsletter for a discussion of the call and go here for the CARB-X webpage on the call. The first cycle is now closed (it ran16-30 April 2025); the 2nd round will be open 1-12 Dec 2025.
- BARDA’s long-running BAA (Broad Agency Announcement) for medical countermeasures (MCMs) for chemical, biological, radiological, and nuclear (CBRN) threats, pandemic influenza, and emerging infectious diseases is now BAA-23-100-SOL-00004 and offers support for both antibacterial and antifungal agents (as well as antivirals, antitoxins, diagnostics, and more). Note especially these Areas of Interest: Area 3.1 (MDR Bacteria and Biothreat Pathogens), Area 3.2 (MDR Fungal Infections), and Area 7.2 (Antibiotic Resistance Diagnostics for Priority Bacterial Pathogens). Although prior BAAs used a rolling cycle of 4 deadlines/year, the updated BAA released 26 Sep 2023 has a 5-year application period that ends 25 Sep 2028 and is open to applicants regardless of location: BARDA seeks the best science from anywhere in the world! See also this newsletter for further comments on the BAA and its areas of interest.
- HERA Invest was launched August 2023 with €100 million to support innovative EU-based SMEs in the early and late phases of clinical trials. Part of the InvestEU program supporting sustainable investment, innovation, and job creation in Europe, HERA Invest is open for application to companies developing medical countermeasures that address one of the following cross-border health threats: (i) Pathogens with pandemic or epidemic potential, (ii) Chemical, biological, radiological and nuclear (CBRN) threats originating from accidental or deliberate release, and (iii) Antimicrobial resistance (AMR). Non-dilutive venture loans covering up to 50% of investment costs are available. A closing date is not posted insofar as I can see — applications are accepted on a rolling basis; go here for more details.
- The AMR Action Fund is open on an ongoing basis to proposals for funding of Phase 2 / Phase 3 antibacterial therapeutics. Per its charter, the fund prioritizes investment in treatments that address a pathogen prioritized by the WHO, the CDC and/or other public health entities that: (i) are novel (e.g., absence of known cross-resistance, novel targets, new chemical classes, or new mechanisms of action); and/or (ii) have significant differentiated clinical utility (e.g., differentiated innovation that provides clinical value versus standard of care to prescribers and patients, such as safety/tolerability, oral formulation, different spectrum of activity); and (iii) reduce patient mortality. It is also expected that such agents would have the potential to strongly address the likely requirements for delinked Pull incentives such as the UK (NHS England) subscription pilot and the PASTEUR Act in the US. Submit queries to contact@amractionfund.com.
- INCATE (Incubator for Antibacterial Therapies in Europe) is an early-stage funding vehicle supporting innovation vs. drug-resistant bacterial infections. The fund provides advice, community, and non-dilutive funding (€10k in Stage I and up to €250k in Stage II) to support early-stage ventures in creating the evidence and building the team needed to get next-level funding. Details and contacts on their website (https://www.incate.net/).
- These things aren’t sources of funds but would help you develop funding applications
- The Global AMR R&D Hub’s dynamic dashboard (link) summarizes the global clinical development pipeline, incentives for AMR R&D, and investors/investments in AMR R&D.
- Antimicrobial Resistance Research and Innovation in Australia is an actively updated summary that covers Australia’s AMR research and patent landscape. It is provided via collaboration between The Lens (an ambitious project seeking to discover, analyse, and map global innovation knowledge) and CSIRO (Commonwealth Scientific and Industrial Research Organisation, an Australian Government agency responsible for scientific research). Lots to explore here!
- Diagnostic developers would find valuable guidance in this 6-part series on in vitro diagnostic (IVD) development. Sponsored by CARB-X, C-CAMP, and FIND, it pulls together real-life insights into a succinct set of tutorials.
- In addition to the lists provided by the Global AMR R&D Hub, you might also be interested in my most current lists of R&D incentives (link) and priority pathogens (link).