Dear All (and with thanks to Arjun Srinivasan for co-authoring this wonkish newsletter — prepare yourself! Know also that we’ve written a parallel newsletter entitled “Economic modeling of the value of rapid diagnostics” that discusses the use of modeling to estimate the value of diagnostics in general):
Driven by ongoing work to encourage use as part of good medical practice and stewardship, discussions of the value of diagnostics have been increasingly prominent in past issues of this newsletter:
- 18 Jun 2025: “Extending STEDI to diagnostics: STRIDES”
- 4 Oct 2025: “WHO: Reviews of antibacterial therapeutics and diagnostics”
- 17 Feb 2026: “Workshop on diagnostics: Can we drive use by making value visible?”
- 9 Apr 2026: “GO-Dx: Global One Health Diagnostics Access Compact”
While a lot of this discussion is focused on simply ensuring access to diagnostics (any diagnostic!), the push for use of diagnostics would be greatly aided by data showing that their use makes a difference in clinical outcomes and improved health system efficiencies. And as a build on that, the idea that rapid initiation of effective therapy improves outcomes drives a push for rapid AST. It would all seem to make perfect sense: the mortality of serious infections can be reduced by an effective antibiotic and this would imply benefits from rapid adjustments to antibiotic therapy (if needed).
Perhaps surprisingly, however, studies of the value of rapid AST have consistently struggled to demonstrate this theoretical value. A recently published study sponsored by the ARLG (Antibiotic Resistance Leadership Group) was both a very good effort to generate such data and a demonstration of the limitations on randomized demonstrations of the utility of diagnostics. To follow the discussion, here are the links you need:
- Papers evaluating the clinical impact of rapid AST methods:
- Banerjee R et al. Fast Antimicrobial Susceptibility Testing for Gram-Negative Bacteremia: The FAST Randomized Clinical Trial. JAMA. 2026, doi: 10.1001/jama.2026.5487. This article prompted this newsletter. It concludes that “Among patients with gram-negative bacilli BSIs, rapid blood culture AST was not superior to standard testing by DOOR.”
- Srinivasan A. A Multinational Trial of Rapid Antimicrobial Susceptibility Testing: Is FASTer Better? JAMA. 2026, doi: 10.1001/jama.2026.5504. Accompanying editorial by Arjun, co-author of this newsletter.
- Anton-Vazquez V et al. Rapid versus standard antimicrobial susceptibility testing to guide treatment of bloodstream infection. Cochrane Database Syst Rev. 2021, doi: 10.1002/14651858.cd013235.pub2. A Cochrane review that concludes “The theoretical benefits of rapid susceptibility testing have not been demonstrated to directly improve mortality, time-to-discharge, or time-to-appropriate antibiotic in these randomized studies.”
- A comparison of six recent prospective studies of rapid AST (Antimicrobial Susceptibility Testing) methods. With Banerjee 2026, there are six such studies. This is a comparative summary that John generated with the assistance of one of the AI models.
- Papers evaluating the clinical impact of delayed antibiotic therapy:
- Kumar A. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med. 2006;34(6):1589–96, doi: 10.1097/01.ccm.0000217961.75225.e9. A classic paper on this topic – one of my favorites.
- Zasowski EJ et al. A Systematic Review of the Effect of Delayed Appropriate Antibiotic Treatment on the Outcomes of Patients with Severe Bacterial Infections. Chest. 2020;158(3):929–38, doi: 10.1016/j.chest.2020.03.087. A recent, well-written systematic review of the literature on this topic.
- Papers evaluating the impact of parachutes on gravitational injury:
- What? Yes, you read that correctly — this is not an April Fool’s Day joke or a review from The Onion! We’ll make use of these papers when get to topics 2 and 3, below!
- Smith GCS, Pell JP. Parachute use to prevent death and major trauma related to gravitational challenge: Systematic review of randomised controlled trials. BMJ. 2003;327:1459–61, doi: 10.1136/bmj.327.7429.1459. No surprise — a systematic review failed to find any RCTs showing that parachutes work.
- Yeh RW et al. Parachute use to prevent death and major trauma when jumping from aircraft: randomized controlled trial. BMJ. 2018, doi: 10.1136/bmj.k5094. To address the gap identified by Smith & Pell, we’ll see that Yeh et al. conducted an RCT … details below!
So, we’re off on a tour of these 3 topics:
- Why did Banerjee 2026 conclude that “Among patients with gram-negative bacilli bloodstream infections, rapid blood culture AST was not superior to standard testing by DOOR.”?
- So, does time to prompt initiation of antimicrobial therapy actually matter?
- What does all this say about showing superiority outcomes in studies of AST (whether rapid or not) and of antimicrobial agents?
Here we go!
Topic 1: Why did Banerjee 2026 conclude that “Among patients with gram-negative bacilli bloodstream infections, rapid blood culture AST was not superior to standard testing by DOOR.”?
The study by Banerjee 2026 was a substantial and well-considered effort to show the value of rapid AST. Building on challenges with prior studies, its key features were:
- It was an open-label randomized clinical trial comparing rapid AST with standard AST as guidance for antibiotic therapy in patients with bloodstream infection due to Gram-negative bacilli (E. coli, etc.)
- It was conducted at 7 medical centers in countries with a high endemicity for resistant organisms: Greece (2), India (1), Israel (3), and Spain (1).
- It was a big study: it randomized 850 subjects: 413 to rapid AST, 437 to standard AST
- Rather than a blunt endpoint of all-cause mortality, its primary outcome was focused on overall clinical response by use of a desirability of outcome ranking (DOOR, Evans 2015) at day 30 based on 3 categories that are ranked from better to worse: (i) alive without deleterious events, (ii) alive with deleterious events, and (iii) death.
Frustratingly, the authors found that:
- Rapid AST did not improve the likelihood of a more favorable DOOR category outcome.
- Rapid AST did reduce the time to antibiotic escalation or de-escalation, but
- … there was no difference in time to effective antibiotic therapy.
The lack of impact of rapid AST on time to effective antibiotic therapy is almost certainly the core issue and can be seen in Figure 4 from the paper where we have antibiotic therapy over time for the two groups. The bottom two bars in each column (purple and blue) are the roll-up of overtreatment (purple) and appropriate treatment (blue): both would be expected to be effective, of course:

To make it a little easier to see, this next figure shows the sum of appropriate treatment + overtreatment (the purple and blue bars, above. As you can see, the % on adequate therapy was essentially identical over time:
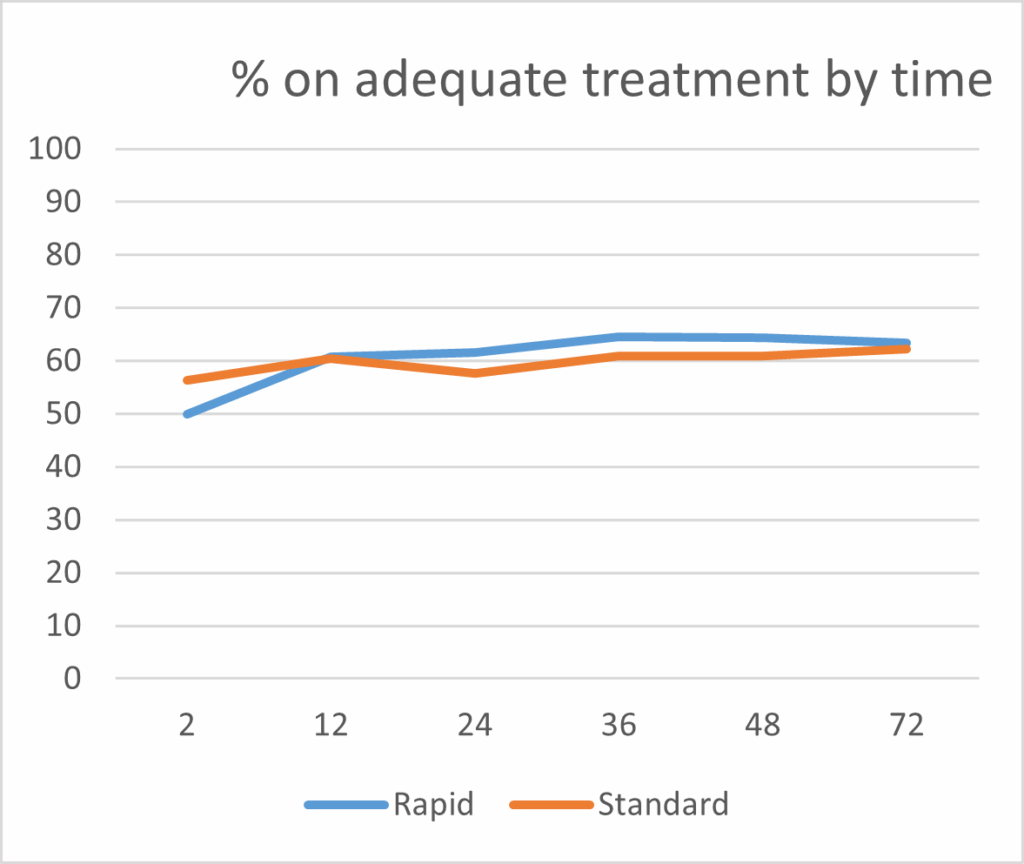
So, that explains the lack of impact of rapid AST … effective antibiotics were used essentially equally well in both arms — or equally poorly, with INappropriate antibiotics used about 40% of the time! Eh? What is going on?
Well, the answer turns out to be related to the theme of these prior newsletters in which we explored the lack of use of newer (less toxic) antibiotics:
- 24 Apr 2026: “DTR Gram-negative infections: Are new antibiotics making a difference?”
- 1 Dec 2024: “The 6 meanings of ‘Lack of Access’ (UNSLAP)”
- 7 Apr 202: “UNSLAP: You reach for the antibiotic … and it’s not there!”
While there are multiple contributing factors (most importantly, rapid molecular ASTs do not [and cannot] detect all forms of resistance), a fundamental issue noted by the authors in their discussion is the lack of access to newer (less toxic agents). Better (rapid) AST is useless if no action is possible!
As a further concern, prior analyses (e.g., Vogler S et al. Health Policy OPEN. 2024;7:100129, doi: 10.1016/j.hpopen.2024.100129) have found that modification of provider behavior requires substantial educational efforts. The manuscript does indicate that the antibiotic stewardship team at each institution would contact the provider if treatment changes were thought needed but it’s not clear how readily or rapidly that advice was utilized at the study sites.
Finally, and further obscuring any potential impact of rapid AST, over half of the subjects had infections due to organisms that were NOT highly resistant thus, they received appropriate therapy without difficulty. Stated differently, if therapy is already appropriate, rapid AST might permit de-escalation but can’t be expected to produce clinical improvement. And it thus follows that measurement of the strength of benefit from rapid AST in the subset really needing AST was diluted by / obscured by the larger pool of patients who received acceptable therapy as part of standard practice.
In summary, and although this trial did find process benefits such as reductions in time to first antibiotic change, the negative result of this trial is readily understood from lack of the ability of an AST (whether rapid or not) to alter selection of (and time to) administration of an appropriate antibiotic unless that antibiotic is available and unless providers are also motivated to act on new data. There are also practical limits on the impact of AST devices, but the foremost problem is that the better agents were often either not available or not used in the study sites!
—–
Topic 2: So, does time to prompt initiation of antimicrobial therapy actually matter? (And we’re soon going to use the bit about gravitational injury — hang in there!)
So, what does this say about the value of AST, whether rapid or not? Well, that’s a separate issue from the impact of initiation of antimicrobial therapy. Overall, there’s little doubt that prompt administration of an effective antibiotic makes a difference … and that lack of effective therapy causes bad outcomes.
The primary data on the impact of early therapy is the extensive observational literature cited above. One can also point at specific bits of data such as the impact of a single prior dose of an effective therapy early in the course of community-acquired bacterial pneumonia (Pertel et al. Effects of prior effective therapy on the efficacy of daptomycin and ceftriaxone for the treatment of community-acquired pneumonia. CID 2008;46(8):1142–51, doi: 10.1086/533441).
And if you want more proof, this population-level figure showing the case fatality rate for erysipelas (a skin infection) in Norway illustrates the dramatic effect of the introduction of first sulfas and then penicillin:
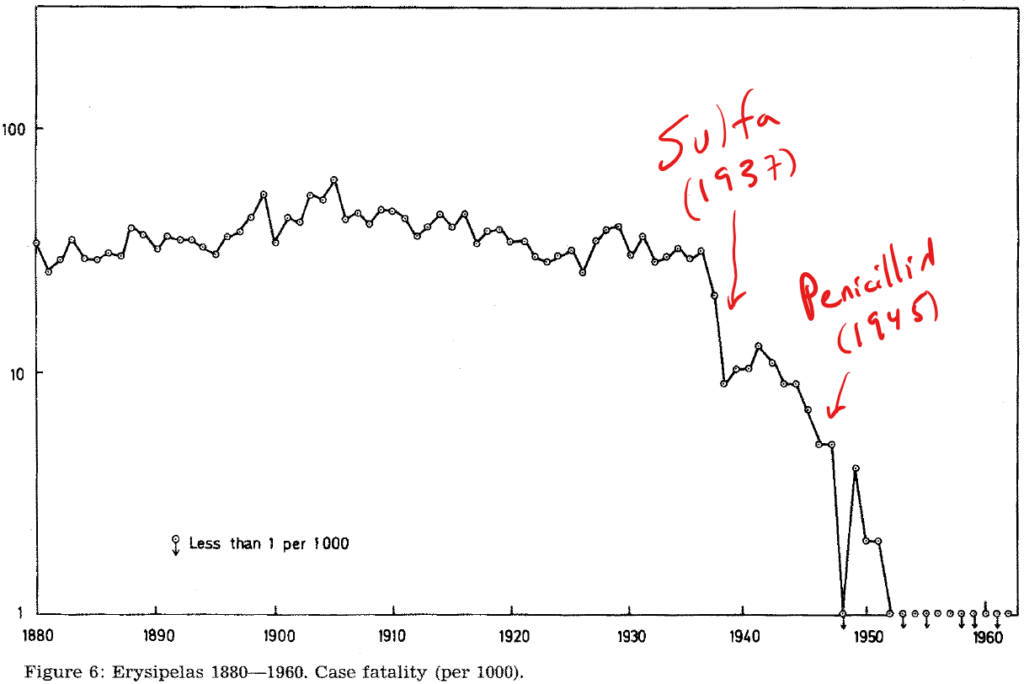
Source: Figure 6 from Madsen ST. Scarlet fever and erysipelas in Norway during the last hundred years. Infection. 1973;1(2):76–81, https://doi.org/10.1007/bf01638479. Note the timescale on the x-axis (1880 to 1960): mortality fell from a steady rate of 20-50/1,000 cases to < 1 death per million cases from the mid-1950s.
While the effect might be less dramatic in LMICs with limited medical resources (see the final paper by the UK AMR Review in May 2016), all serious infections progress through stages of clinical severity. Inevitably, there is a point at which it doesn’t look so bad, then it’s a bit worse, and then it’s awful, and finally it’s too late. This is obvious on its face from the pathophysiology of disease and is supported by the personal experience of anyone who’s cared for such patients.
And it’s here (finally!) that the two papers on parachutes to prevent gravitational injury become relevant. The first (Smith 2003) was a snarky commentary on the desire for an RCT for everything and is included mainly for completeness: “As with many interventions intended to prevent ill health, the effectiveness of parachutes has not been subjected to rigorous evaluation by using randomised controlled trials.”
It’s the second paper (Yeh 2018) that provides the key message about feasibility and context for RCTs in some situations. In this study, the authors measured the rate of injury or death following a jump from an aircraft (airplane or helicopter) while wearing either a parachute or an empty backpack. The twist was that the jump was from an aircraft that was parked. On the ground. Not moving. Thus (and no surprise), this randomized study of 23 subjects found that:
- “Parachute use did not reduce death or major traumatic injury when jumping from aircraft in the first randomized evaluation of this intervention.
- “However, the trial was only able to enroll participants on small stationary aircraft on the ground, suggesting cautious extrapolation to high altitude jumps.”
OK … so that’s pretty snarky … but the point is that demonstrations of superiority require a plausible difference in outcomes between the arms. At the same time, we must also always protect study subjects to the maximum extent possible, and so there are limits on plausible designs. Like the parachute study, the circumstances at Banerjee’s study sites were such that it can be seen (in retrospect) that the lack of plausible scope for improvement in most subjects obscured any improvement in the subset of patients who actually could have benefited.
And we now need to connect this idea to topic 3…
—–
Topic 3: What does all this say about showing superiority outcomes in studies of (i) AST (whether rapid or not) and (ii) antimicrobial agents?
Following on from parachutes in Topic 2, we now need to loop back to a perennial question: Why don’t we routinely have randomized superiority data on novel anti-infective agents or AST? And actually, is it even plausible to expect to have such data?
Hopefully, you’ll now understand that the answer is “No, not unless something really bad has happened!” Good (and ethical) medical practice in studies of potentially lethal infections demands that we always ensure that we are trying to deliver effective therapy to participants in both arms.
With respect to this idea for trials of novel therapies, please review these sources:
- Nambiar S, Laessig K, Toerner J, Farley J, Cox E. Antibacterial drug development: challenges, recent developments, and future considerations. Clin Pharmacol Ther. 2014;96(2):147–9, doi: 10.1038/clpt.2014.116. An excellent discussion by five colleagues from FDA of the issues with doing superiority studies.
- 19 Sep 2020 newsletter: “In praise of non-inferiority” This newsletter, along with its associated YouTube explainer, provides a deep dive into the tension between superiority studies and non-inferiority studies.
And for AST (whether rapid or not), the exceptional effort by Banerjee et al. to produce such data is noteworthy and instructive. As discussed in the primary paper and the accompanying editorial, it might be possible to find a subset in which a difference could be shown, but (from Arjun’s editorial):
- “…trying to focus rapid AST on a subset of patients where it might have clear mortality benefit seems impractical and unnecessary.
- “Nearly every hospital in the US, and many globally (including all the hospitals in the FAST trial), have antibiotic stewardship programs focused on ensuring that patients receive optimal antibiotic therapy.
- “If we have a tool that will help antibiotic stewardship programs support clinicians in optimizing therapy faster, an outcome that is consistent across all studies of rapid AST, should we not work toward making that tool available?
- “The answer from a patient-centric perspective is clearly yes.”
—
In summary, our ability to measure the differential impact of more rapid forms of AST is always going to be limited. A difference is certain to exist for patients with rapidly progressive, severe forms of infection but modern therapeutic approaches work to reduce such differences. Further, it just doesn’t make sense to try to triage use of rapid AST as infections that seem mild at the start can progress very rapidly to death.
Thus, arguments around use of (rapid) AST will need to be built around economic modeling of the cost and value of different approaches. On that point, see the parallel newsletter entitled “Economic modeling of the value of rapid diagnostics”!
Best wishes,
John & Arjun
John H. Rex, MD | Chief Medical Officer, F2G Ltd. | Operating Partner, Advent Life Sciences. Follow me on Twitter: @JohnRex_NewAbx. See past newsletters and subscribe for the future: https://amr.solutions/blog/. All opinions are my own.
Arjun Srinivasan, MD | Deputy Chief Medical Officer, Joint Commission | formerly, Deputy Director, Division of Healthcare Quality Promotion, US CDC | Follow me at linkedin.com/in/arjun-srinivasan-28951b355. All opinions are my own.
John’s Top Recurring Meetings
Virtual meetings are easy to attend, but regular attendance at annual in-person events is the key to building your network and gaining deeper insight. My personal favorites for such in-person meetings are below. Of particular value for developers, the small meeting format of BEAM’s AMR Conference (March) and GAMRIC (September-October; formerly, the ESCMID-ASM conference series) creates excellent global networking. IDWeek (October) and ECCMID (April) are much larger meetings but also provide opportunities for networking with a substantial, focused audience via their Pipeline sessions. Hope to see you there!
- [UPDATED INFO] 22-24 Sep 2026 (Lisbon, Portugal): The 2nd GAMRIC, the Global AMR Innovators Conference (London, UK). Formerly the ESCMID-ASM (or ASM-ESCMID depending on location) Joint Conference on Drug Development for AMR, 2026 will be the 11th year for this series that is now under the joint sponsorship of CARB-X, ESCMID, BEAM Alliance, GARDP, LifeArc, Boston University, and AMR.Solutions. The ongoing series employs the successful format of prior meetings with a single-track meeting and substantial networking time. The 2025 meeting was a sell-out success: a written summary is here and the videos are here. Registration for the 2026 meeting is now open and the near-final program is here: in addition to a keynote lecture by Karen Bush on the threat to beta-lactams due to the emergence of PBP3 mutations, there are sessions on funding, access, program design for narrow-spectrum agents such as phage, development for pediatrics, and more. The main abstract submission window is closed but late-breaker abstracts will be accepted 8-22 July 2026.
- 21-24 Oct 2026 (Washington, DC, USA): IDWeek 2026, the annual meeting of the Infectious Diseases Society of America. I would expect the program to continue to provide a substantial opportunity to present a product to a large audience (see also adjacent note about ESCMID) as well as opportunities to present at an IDWeek Pipeline Session.
- 23-24 Mar 2027 (Basel, Switzerland): The 10th AMR Conference (3-4 Mar 2026) is now over and offered a rich program that included a 10-year retrospective (we’ve done a lot!), regulatory updates, discussions of how to pursue development in China, and much more … in addition to being a superb opportunity for networking! I am told the session videos will soon be available on the conference website.
- 9-13 April 2027 (Stockholm, Sweden): ESCMID Global 2027, the annual meeting of the European Society for Clinical Microbiology and Infectious Diseases. Details won’t be out for some months, but the website is here. I do know that the meeting schedule will again include a Science Policy Forum on Friday 9 April 2027 (see here the newsletter about the 2026 science policy forum) and all who are interested in Pull incentives and the antibiotic ecosystem should plan to be there!)..
Upcoming meetings of interest to the AMR community:
- 4-8 June 2026 (Washington, DC): ASM Microbe, the annual meeting of the American Society for Microbiology. The meeting format is evolving and next year will combine 3 meetings (ASM Health, ASM Applied and Environmental Microbiology, and ASM Mechanism Discovery) into one event. Go here for details.
- 11-12 Jun 2026 (Washington, DC): The Second Annual Unite for Sepsis Symposium, presented by the Sepsis Alliance. The event seeks to accelerate progress in sepsis research and care. Go here for details and to register.
- 22-24 Sep 2026 GAMRIC (Lisbon, Portugal), the Global AMR Innovators Conference (London, UK; formerly the ESCMID-ASM Joint Conference on Drug Development for AMR). See list of Top Recurring meetings, above..
- [REGISTRATION IS OPEN] 10-18 Oct 2026 (Annecy, France, residential in-person program): ICARe (Interdisciplinary Course on Antibiotics and Resistance) … and 2026 will be the 10th year for this program. Patrice Courvalin orchestrates content with the support of an all-star scientific committee and faculty. The resulting soup-to-nuts training covers all aspects of antimicrobials, is very intense, and routinely gets rave reviews! Registration for 2026 is now open and runs through June 21, 2026. Go here to register!
- 21-24 Oct 2026 (Washington, DC, USA): IDWeek 2026. See list of Top Recurring meetings, above.
- 10-13 November 2026 (Madrid, Spain): The International Society for Infectious Diseases (ISID) has announced its 21st International Congress on Infectious Diseases (ICID). Register and view the preliminary program here (Early bird closes 30 July 2026); abstract deadline is 28 April 2026.
- 23-24 Mar 2027 (Basel, Switzerland): The 11th AMR Conference sponsored by the BEAM Alliance. See list of Top Recurring meetings, above.
- 9-13 April 2027 (Stockholm, Sweden): ESCMID Global 2026, the annual meeting of the European Society for Clinical Microbiology and Infectious Diseases. See Recurring Meetings list, above.
- ??? Mar 2028 (yes, that’s 2028, with location TBD): The 2028 Gordon Research Conference (GRC, https://www.grc.org/) entitled “Antibacterials of Tomorrow to Combat the Global Threat of Antimicrobial Resistance” and its related Gordon Research Seminar (GRS) for young doctoral and post-doctoral researchers will be sometime in March 2028. The organizers hope to coordinate dates and location with the 2028 BEAM-AMR meeting. Details to follow — mark your calendar!
Self-paced courses, online training materials, and other reference materials:
- OpenWHO: “Antimicrobial Resistance in the environment: key concepts and interventions.” Per the webpage for the course, it will teach you “…why addressing AMR in the environment is essential and gain insights into how action can be taken to prevent and control AMR in the environment at the national level.” This course builds on WHO’s 2024 Guidance on wastewater and solid waste management for manufacturing of antibiotics. For further reading, see also the 25 Sep 2023 newsletter entitled “Manufacturing underpins both access and stewardship: Cefiderocol as a case study” and the 28 Jan 2024 newsletter entitled “EMA Concept Paper: Guidance on manufacturing of phage products”.
- GARDP’s REVIVE website provides an encyclopedia covering a range of R&D terms, recordings of prior GARDP webinars, a variety of viewpoint articles, and more! Check it out!
- GARDP’s https://antibioticdb.com/ is an open-access database of antibacterial agents.
- The CARB-X website provides a range of recordings from its webinars, bootcamps, and more. A bit of browsing would be time well spent!
- British Society for Antimicrobial Chemotherapy offers an eLearning section: Education – The British Society for Antimicrobial Chemotherapy.
- CARB-X have had one funding round (8-22 April 2026); a further round is expected during 4Q 2026. There are 4 funding themes for these rounds as below.
- Direct-acting therapeutics for infections caused by Gram-negative bacteria
- Novel Chemistry for AMR Challenge – target-based therapeutics.
- Non-vaccine approaches to prevent neonatal sepsis
- Diagnostics for neonatal sepsis
- The Horizon Europe Work Programme 2026-2027 includes at least 3 calls of interest within its Cluster 1 — see the list below. The application window starts 10 Feb 2026 and closes on 16 Apr 2026. See also the 12 Dec 2025 newsletter about the call. Note as well that there calls for agents to prevent and/or treat viral infections.
- HORIZON-HLTH-2027-01-DISEASE-08: Development of innovative antimicrobials against pathogens resistant to antimicrobials
- HORIZON-HLTH-2027-02-IND-02: Portable point-of-care diagnostics
- HORIZON-HLTH-2026-01-DISEASE-03:Advancing research on the prevention, diagnosis, and management of post-infection long-term conditions.
- ENABLE-2 has continuously open calls for both its Hit-to-Lead program as well as its Hit Identification/Validation incubator. Applicants must be academics and non-profits in Europe due to restrictions from the funders. Applications are evaluated in cycles … see the website for details on current timing for reviews.
- BARDA’s long-running BAA (Broad Agency Announcement) for medical countermeasures (MCMs) for chemical, biological, radiological, and nuclear (CBRN) threats, pandemic influenza, and emerging infectious diseases is now BAA-23-100-SOL-00004 and offers support for both antibacterial and antifungal agents (as well as antivirals, antitoxins, diagnostics, and more). Note especially these Areas of Interest: Area 3.1 (MDR Bacteria and Biothreat Pathogens), Area 3.2 (MDR Fungal Infections), and Area 7.2 (Antibiotic Resistance Diagnostics for Priority Bacterial Pathogens). Although prior BAAs used a rolling cycle of 4 deadlines/year, the updated BAA released 26 Sep 2023 has a 5-year application period that ends 25 Sep 2028 and is open to applicants regardless of location: BARDA seeks the best science from anywhere in the world! See also this newsletter for further comments on the BAA and its areas of interest.
- HERA Invest was launched August 2023 with €100 million to support innovative EU-based SMEs in the early and late phases of clinical trials. Part of the InvestEU program supporting sustainable investment, innovation, and job creation in Europe, HERA Invest is open for application to companies developing medical countermeasures that address one of the following cross-border health threats: (i) Pathogens with pandemic or epidemic potential, (ii) Chemical, biological, radiological and nuclear (CBRN) threats originating from accidental or deliberate release, and (iii) Antimicrobial resistance (AMR). Non-dilutive venture loans covering up to 50% of investment costs are available. A closing date is not posted insofar as I can see — applications are accepted on a rolling basis; go here for more details.
- The AMR Action Fund is open on an ongoing basis to proposals for funding of Phase 2 / Phase 3 antibacterial therapeutics. Per its charter, the fund prioritizes investment in treatments that address a pathogen prioritized by the WHO, the CDC and/or other public health entities that: (i) are novel (e.g., absence of known cross-resistance, novel targets, new chemical classes, or new mechanisms of action); and/or (ii) have significant differentiated clinical utility (e.g., differentiated innovation that provides clinical value versus standard of care to prescribers and patients, such as safety/tolerability, oral formulation, different spectrum of activity); and (iii) reduce patient mortality. It is also expected that such agents would have the potential to strongly address the likely requirements for delinked Pull incentives such as the UK (NHS England) subscription pilot and the PASTEUR Act in the US. Submit queries to contact@amractionfund.com.
- INCATE (Incubator for Antibacterial Therapies in Europe) is an early-stage funding vehicle supporting innovation vs. drug-resistant bacterial infections. The fund provides advice, community, and non-dilutive funding (€10k in Stage I and up to €250k in Stage II) to support early-stage ventures in creating the evidence and building the team needed to get next-level funding. Details and contacts on their website (https://www.incate.net/).
- These things aren’t sources of funds but would help you develop funding applications
- The Global AMR R&D Hub’s dynamic dashboard (link) summarizes the global clinical development pipeline, incentives for AMR R&D, and investors/investments in AMR R&D. See also the 7 Feb 2026 newsletter (“The global funding pipeline, 2017-2023: A review”) about an excellent deep dive by the Hub team into patterns of funding over time.
- Antimicrobial Resistance Research and Innovation in Australia is an actively updated summary that covers Australia’s AMR research and patent landscape. It is provided via collaboration between The Lens (an ambitious project seeking to discover, analyse, and map global innovation knowledge) and CSIRO (Commonwealth Scientific and Industrial Research Organisation, an Australian Government agency responsible for scientific research). Lots to explore here!
- Diagnostic developers would find valuable guidance in this 6-part series on in vitro diagnostic (IVD) development. Sponsored by CARB-X, C-CAMP, and FIND, it pulls together real-life insights into a succinct set of tutorials.
- In addition to the lists provided by the Global AMR R&D Hub, you might also be interested in my most current lists of R&D incentives (link) and priority pathogens (link).